A parent recently asked me whether shoulder dystocia can affect a child’s vision.
The good news is that most children who experience shoulder dystocia will never develop vision problems. However, in some severe birth injury cases, vision-related complications can occur.
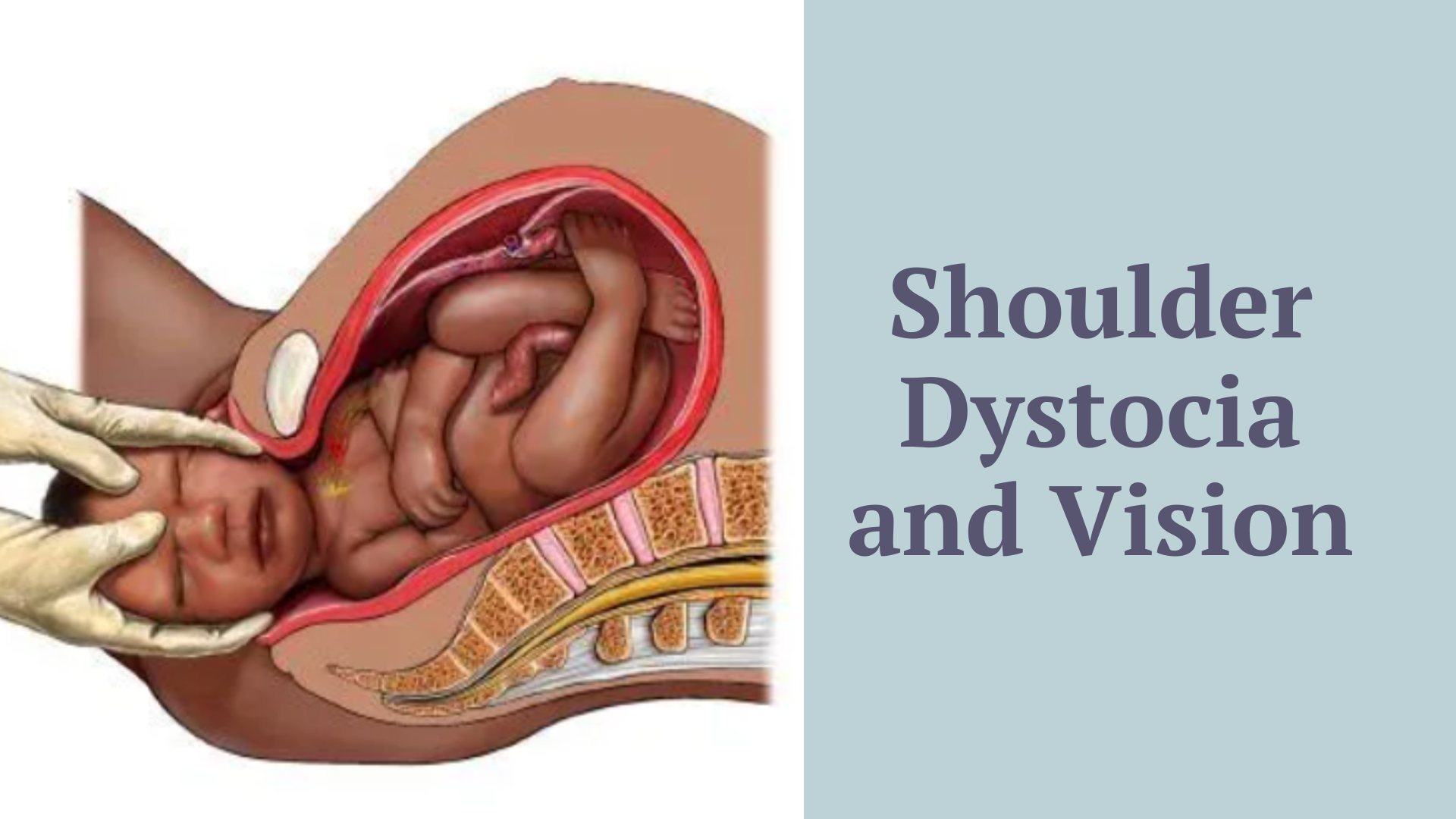
Shoulder dystocia is an obstetric emergency that occurs when a baby’s head is delivered but one or both shoulders become trapped behind the mother’s pelvic bone.
In some of the more severe shoulder dystocia cases I’ve reviewed, two vision-related diagnoses that have emerged are Horner Syndrome and Cerebral Visual Impairment (CVI).
If your child experienced a difficult birth and you are now noticing unusual visual behaviors or asymmetries in their eyes, it is important to discuss these concerns with your medical team.
1. Horner Syndrome: The Link Between Nerve Damage and the Eye
Horner syndrome is not typically an injury to the eye itself. Instead, it is a neurological condition caused by an injury to the sympathetic nerve pathway, the nerve network that controls involuntary functions like pupil dilation and eyelid movement.
According to clinical data from Boston Children’s Hospital, Horner syndrome occurs in roughly 10% to 20% of brachial plexus injuries. When these nerves are damaged during a difficult shoulder dystocia delivery, it often signals a highly severe brachial plexus injury, such as an avulsion (where the nerve is completely torn from the spinal cord).
Signs Parents May Notice:
- Smaller Pupil: One pupil looks noticeably smaller than the other.
- Drooping Eyelid: One eyelid droops slightly, making the baby’s eyes look uneven or asymmetrical.
- Decreased Sweating: Decreased or absent sweating on one side of the baby’s face.
The Long-Term Impact on Vision
Most of the time, Horner syndrome affects the appearance and function of the eyelid and pupil rather than vision itself. Many children retain normal sight, though medical teams must monitor them closely; if the eyelid droops severely enough to block the pupil entirely, it can interfere with the child’s early visual development.
Treatment heavily depends on the underlying brachial plexus injury. While stretched nerves can heal through targeted physical therapy, severe avulsions cannot be repaired directly and may require advanced microsurgery, such as nerve grafts or nerve transfers, ideally performed between 3 and 9 months of age.
2. Cerebral/Cortical Visual Impairment (CVI): When the Brain Cannot “See”
While Horner syndrome stems from physical nerve trauma in the neck, another vision-related complication can arise from a completely different mechanism during shoulder dystocia: oxygen deprivation.
In a child with CVI, the eyes themselves are often structurally normal. The issue lies in the brain’s visual processing centers. CVI is diagnosed when abnormal visual responses cannot be attributed to the eyes, eye movements, or simple refractive errors. Today, it stands as the most common cause of permanent visual impairment in children. Because CVI affects how the brain processes visual information, it can influence learning, mobility, communication, and daily functioning even when a child’s eyesight appears normal.
The Connection to Delivery Complications
CVI occurs when there is an injury to the brain’s bilateral, post-chiasmal visual pathways, which include both the gray matter (cortical) and white matter (subcortical) regions.
In severe shoulder dystocia cases, prolonged umbilical cord compression or impaired oxygen delivery can contribute to hypoxic-ischemic injury. One recognized cause of CVI in children is Hypoxic-Ischemic Encephalopathy (HIE), a type of brain injury caused by insufficient oxygen and blood flow.
Because the brain’s visual processing networks are highly sensitive to oxygen loss, HIE can affect these pathways even when the physical structures of the eyes remain completely normal.
Signs Parents May Notice:
Because CVI affects how the brain interprets data, its symptoms manifest as distinct behavioral traits rather than physical changes in the eye’s appearance. Clinical resources outline several common signs:
- Inconsistent Visual Responses: A child may look at an object one day and ignore it the next. They often respond much better to familiar items than new ones.
- Blunted or Avoidant Social Gaze: Parents are often deeply concerned by a lack of direct eye contact. A child with CVI may actively look away from or withdraw from faces.
- Difficulty with “Visual Crowding”: The child may struggle to see an object if it is placed against a busy, colorful background or in a crowded array.
- Preference for Movement and Color: Many children show a strong preference for highly saturated colors (like bright red or yellow) and can track moving objects much better than static ones.
- Sensory Overload: A child’s ability to use their vision may drop significantly if the environment is noisy, if people are speaking, or if they are being touched. They often “fatigue” quickly from visual tasks.
- Reaching Without Looking: A child with motor capabilities might reach out to touch an object using their peripheral vision or purely by touch, without looking directly at it.
Protecting Your Child’s Future: Medical and Legal Support
Both Horner syndrome and CVI are rare complications that are generally associated with only the most severe cases of shoulder dystocia. Fortunately, the vast majority of babies are delivered safely without any permanent harm.
However, if you are noticing any unusual symptoms, such as a drooping eyelid, uneven pupils, a lack of eye contact, or tracking issues, it is worth raising these concerns with your child’s medical team right away. Managing these complex conditions requires early identification and specialized care to support your child’s development.
In some circumstances, families may have questions about whether different medical decisions or interventions could have altered the outcome. When serious birth injuries occur, families are often left navigating unexpected medical, financial, and emotional challenges.
Disclaimer
Legal and Medical Disclaimer: The information provided in this article is for educational and informational purposes only and does not constitute legal or medical advice. Reading this article does not establish an attorney-client relationship with Liro Willer Law. While this content discusses evolving medical standards of care and potential legal frameworks, medical malpractice determinations are highly fact-specific and vary by jurisdiction. Individuals seeking medical diagnosis or treatment should consult a licensed healthcare professional. Individuals seeking legal advice regarding potential medical negligence or malpractice should consult a qualified attorney licensed in their jurisdiction.
References
Boston Children’s Hospital. Brachial Plexus Birth Injury. Retrieved from: [https://www.childrenshospital.org/conditions-treatments/brachial-plexus-birth-injury]
Boston Children’s Hospital. Cortical Visual Impairment. Retrieved from: [https://www.childrenshospital.org/conditions-treatments/cortical-visual-impairment]
Perkins School for the Blind. What is CVI? CVI’s Impact. Retrieved from: https://www.perkins.org/what-is-cvi/#h-cvi-s-impact
Journal of American Association for Pediatric Ophthalmology and Strabismus (JAAPOS). Pediatric Horner Syndrome https://www.jaapos.org/article/S1091-8531(98)90008-8/pdf