
If you’ve been following birth trends, you’ve likely heard of the ARRIVE trial. While this landmark study provided evidence for elective inductions at 39 weeks, recent data suggests that medical practices are “drifting” into much earlier territory, specifically the 37- and 38-week mark, without the same level of evidentiary support as elective induction at 39 weeks.
In this post, we’ll break down a recent analysis of US natality data from 2016 to 2024 and explore why many in the birth world are raising red flags about the normalization of early-term inductions.
What was the ARRIVE Trial?
The ARRIVE trial (A Randomized Trial of Induction Versus Expectant Management) was a large multi-center study designed to determine if inducing healthy, low-risk, first-time mothers at 39 weeks would reduce adverse perinatal outcomes and cesarean delivery rates. The trial randomly assigned 6,106 low-risk nulliparous women to either labor induction at 39 weeks (3,062 women) or expectant management (3,044 women). The study’s key findings included:
- Reduced Cesarean Rates: The frequency of cesarean delivery was significantly lower in the induction group (18.6%) compared to the expectant-management group (22.2%).
- Perinatal Outcomes: There was no significant difference between the groups regarding a composite of perinatal death or severe neonatal complications (4.3% in the induction group vs. 5.4% in expectant management).
- Maternal Health: Women in the induction group had a lower risk of developing hypertensive disorders of pregnancy.
However, the trial was very specific: it looked at a specific population of low-risk, first-time mothers induced specifically between 39 weeks 0 days and 39 weeks 4 days.
The Data: A Trend Toward “Early-Term” Induction
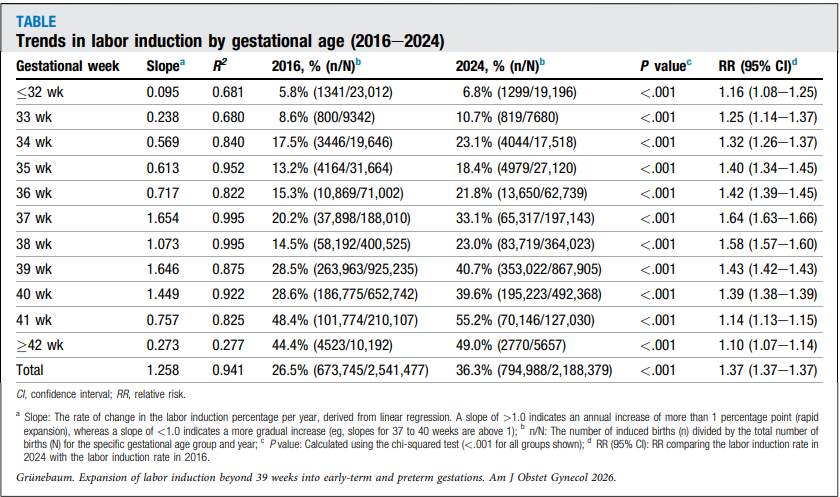
A 2026 research letter published in the American Journal of Obstetrics & Gynecology analyzed US natality data from 2016 to 2024. By excluding pregnancies with major medical indications like prior C-sections, hypertension, or diabetes, researchers attempted to isolate trends in likely non-medically indicated inductions.
Some of the key findings between 2016 -2024 are:
-
Universal Increase: Induction rates increased across all gestational ages over the eight-year period.
-
The 37 & 38-Week Jump: While the ARRIVE trial focused on 39 weeks, the greatest proportional increase in induction rates occurred at 37 and 38 weeks.
-
A Shift in Birth Distribution: As inductions rose, the percentage of deliveries between 37 and 39 weeks jumped significantly, while deliveries at 40 weeks or beyond declined.
Why Is This Happening? “Normalization of Deviance”
The authors suggest the trend may reflect a phenomenon sometimes referred to as ‘normalization of deviance.’ This occurs when an intervention is repeatedly accepted, gradually eroding its original evidentiary boundaries.
Essentially, because the medical community became comfortable with 39-week inductions following the ARRIVE results, the practice began to “drift” earlier into the 37th and 38th weeks. The study notes that the growth at 37–38 weeks suggests these inductions are transitioning from exceptional cases into routine patterns, despite limited randomized evidence demonstrating similar benefits for elective induction before 39 weeks in otherwise low-risk pregnancies.
Induction trends by the numbers
Why Caution is Necessary
The researchers and many birth advocates are calling for a re-examination of these practices. The concern is that clinical comfort with 39-week induction may be extending into earlier gestations where evidence is less established.
Importantly, many inductions before 39 weeks are medically necessary and can be lifesaving for both mother and baby.
If you are currently pregnant or planning a birth, it is essential to ask your provider for the documented medical or obstetrical indication if an induction is recommended before 39 weeks.
What are your thoughts on elective inductions? Have you noticed a shift toward earlier birth dates in your community? Let’s discuss in the comments.
This post is for informational purposes only and does not constitute medical advice. Always consult with your healthcare provider regarding your specific pregnancy and birth plan.
References
Expansion of labor induction beyond 39 weeks into early-term and preterm gestations in the United States, 2016–2024- Amos Grünebaum, MD Frank A. Chervenak, MD
Grobman, W. A., Rice, M. M., Reddy, U. M., Tita, A. T. N., Silver, R. M., Mallett, G., Hill, K., Thom, E. A., El-Sayed, Y. Y., Perez-Delboy, A., Rouse, D. J., Saade, G. R., Boggess, K. A., Chauhan, S. P., Iams, J. D., Chien, E. K., Casey, B. M., Gibbs, R. S., Srinivas, S. K., Swamy, G. K., Simhan, H. N., & Macones, G. A. (2018). Labor induction versus expectant management in low-risk nulliparous women. New England Journal of Medicine, 379(6), 513–523. https://doi.org/10.1056/nejmoa1800566
Carmichael, S. L., & Snowden, J. M. (2019). The ARRIVE trial: Interpretation from an epidemiologic perspective. Journal of Midwifery & Women’s Health, 64(5), 657–663. https://doi.org/10.1111/jmwh.12996
Wennerholm, U. B., Saltvedt, S., Wessberg, A., Alkmark, M., Bergh, C., Wendel, S. B., Fadl, H., Jonsson, M., Ladfors, L., Sengpiel, V., Wesström, J., Wennergren, G., Wikström, A. K., Elden, H., Stephansson, O., & Hagberg, H. (2019). Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEdish Post-term Induction Study, SWEPIS): Multicentre, open label, randomised, superiority trial. BMJ, 367. https://doi.org/10.1136/bmj.l6131
Facchinetti, F., Menichini, D., & Perrone, E. (2020). The ARRIVE trial will not “arrive” to Europe. The Journal of Maternal-Fetal & Neonatal Medicine, 35(22), 4229–4232. https://doi.org/10.1080/14767058.2020.1849128